



If you are or have ever been pregnant, you’d probably just as soon forget the glucose tolerance test used to screen for gestational diabetes. I certainly didn’t enjoy sitting in my OB’s waiting room with a sugar rush before 9 A.M., but I’m even more grateful that I passed the test and my personal experience with gestational diabetes ended there. For an increasing number of women worldwide, gestational diabetes is raising the risk of pregnancy complications and health problems down the road.
Knowing the basics about gestational diabetes—and the best ways to prevent it—could be the key to not having to know more details than you’d like. In this primer, I’ll discuss what gestational diabetes is, how it’s diagnosed, and what you might not hear from your doctor about ways to minimize its effects on both mother and baby.
What is gestational diabetes mellitus (GDM)?
Gestational diabetes (also called gestational diabetes mellitus, or GDM) is defined as hyperglycemia, or high blood sugar, first detected during pregnancy. It’s a type of diabetes that may develop during pregnancy, or there may have been preexisting Type 1 or Type 2 diabetes before pregnancy that had never been diagnosed.
Gestational diabetes affects up to 9% of pregnancies in the U.S. each year and is becoming increasingly common. A 2021 study conducted by Northwestern Medicine found that rates of GDM rose thirty percent between 2011 and 2019 alone [1].
What causes gestational diabetes?
According to the popular pregnancy advice website, Evidence Based Birth, GDM can result from rising hormones from the placenta, making it more difficult for the mother’s body to use insulin. Insulin is the hormone used to process sugar.
In every pregnancy, especially during the second half, the mother’s body develops some level of insulin resistance. This means that cells are not as responsive to insulin and have a harder time removing sugar from the blood. The purpose of preventing cells from absorbing as much sugar is to push as many nutrients as possible towards the developing baby. At the same time, your body’s ideal blood sugar range is about 20% lower than it is when you’re not pregnant. The pancreas responds by producing a lot more insulin to overcome the cells’ insulin resistance and keep blood sugar levels low.
Gestational diabetes occurs when the pancreas can’t make enough insulin to keep up, or when cells are too resistant to the amount being produced. As a result, blood sugar levels become too high.
Why is GDM becoming more prevalent?
The Northwestern Medicine study found that diabetes rates before pregnancy also rose by about 20 percent between 2011 and 2019. The authors of the study point to the parallel rise in obesity rates, lack of exercise, and low-quality diet as the primary reasons for the increase in GDM [1]. Extra body fat tends to increase insulin resistance, so it makes sense that higher rates of obesity, insulin resistance, and prediabetes in the general population are contributing to the rapidly increasing prevalence of GDM. Another recent study tied consumption of ultra-processed foods, specifically to a higher rate of GDM [2].
Maternal age is often also listed as a risk factor for GDM, but the Northwestern Medicine study notes that average maternal age increased by less than two years over the course of the same decade, and that GDM rates rose among all age groups. In other words, women waiting longer to have babies are not a primary cause of the steep rise in GDM.
Gut issues are also on the rise and correlated with GDM; these often underlie PCOS, pregnancy complications, and weight gain.
Risks to both mom and baby
Gestational diabetes is a cause for concern because it comes with risks both during and after the pregnancy, for both the mother and the baby developing in her womb.
For the mother, GDM is linked to a higher risk of high blood pressure, preeclampsia, and a C-section delivery. The most common complications for the baby are large birth weight, low blood sugar, and high insulin levels. Low blood sugar or high insulin levels result because the baby has adapted to receiving high levels of glucose from mom. After delivery, his pancreas continues to produce high levels of insulin. Without the same supply of glucose, insulin removes too much sugar too quickly from his blood.
Other risks for the baby linked to GDM are preterm birth, respiratory distress syndrome, chemical imbalances, congenital heart defects, and stillbirth [3].
Both mothers and babies are significantly more likely to develop type 2 diabetes if a GDM diagnosis is received during pregnancy (more on this later).
Both mothers and babies are significantly more likely to develop type 2 diabetes if a GDM diagnosis is received during pregnancy.
How is GDM diagnosed?
Because insulin resistance naturally increases in the second half of pregnancy, most pregnant women are screened for gestational diabetes between 24 and 28 weeks. Women who are at greater risk for gestational diabetes may be screened during the first trimester. The screening involves taking a glucose tolerance test (GTT): drinking a sugary solution (glucola) and then having blood drawn to measure blood sugar levels. The standard screening method in the US is known as the two-step approach:
Step 1: The mother drinks a solution with 50 grams of glucose (nonfasting). After 1 hour, her blood is drawn to measure blood glucose levels. The exact cutoff for a GDM diagnosis depends on the healthcare practitioner’s preferences, because ACOG allows for a threshold of 130, 135, or 140 mg/dL. For the approximately 9 out of 10 women whose blood sugar reads below the threshold, the process ends here, without a gestational diabetes diagnosis. If her blood sugar level is higher than the threshold, she proceeds to step 2.
Step 2: After fasting for at least 8 hours, the mother drinks a solution with 100 grams of glucose. Blood is drawn before and at 1, 2, and 3 hours after drinking the solution. GDM is diagnosed if at least two of the four blood sugar level readings exceed the following thresholds: 95 mg/dL when fasting, 180 mg/dL after 1 hour, 155 mg/dL after 2 hours, or 140 mg/dL after 3 hours.
Another way that healthcare practitioners may check for gestational diabetes is with a urine test. Though it’s normal for the kidneys to leak sugar into urine from the bloodstream, especially after eating a large meal or drinking something sweet, consistently having high glucose in urine may indicate gestational diabetes. However, a urine test alone is not enough to diagnose GDM; a positive GTT result is still needed to confirm GDM.
Are there alternatives to the glucose tolerance test?
If you’re wary about the GTT simply because the thought of chugging sugar water sounds gross to you, you’re not alone. Several substitutes have been proposed, including jelly beans, fruit juice, or a “test meal” with a high amount of glucose [4]. The problem with these alternatives is that they greatly reduce the dependability of the test because they are not standardized. With the serious complications that can arise from high blood sugar during pregnancy, it’s worth getting an accurate picture of your blood glucose levels.
You can avoid the dyes and preservatives in some types of glucola with a more natural alternative like the Fresh Test. I opted for this when I was pregnant because I had previously done a GTT and disliked the artificial taste of the glucola. My care team had no problem with me using the Fresh Test. I just had to purchase it myself (for about $20) and bring the packet with me on the day of my screening. I definitely preferred the taste, which was more like a very sweet lemonade, to that of the glucola.
What to expect if you receive a GDM diagnosis
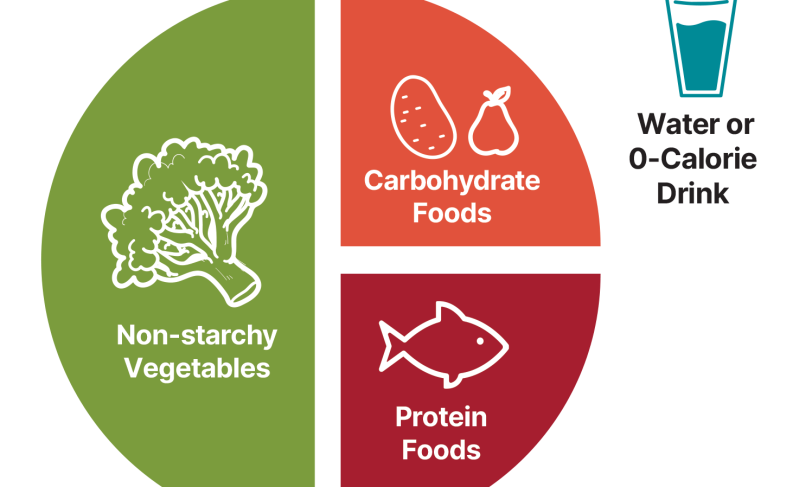
The standard treatment plan for gestational diabetes starts with diet and exercise. Exact guidelines vary depending on the care team, but women diagnosed with gestational diabetes are usually advised to limit the amount of carbohydrates they eat. The ADA’s Diabetes Plate provides a visual guide for an ideal meal: half the meal as non-starchy vegetables, a quarter as protein, and no more than a quarter as carbs.
In addition to “counting carbs,” regularly checking blood sugar levels is usually required. This may involve using a finger prick glucose reader, or wearing a continuous glucose monitor (CGM).
Regular, moderate exercise, five days per week for at least 30 minutes, is also recommended to keep blood sugar in check.
If limiting carb intake and exercising aren’t enough to keep blood sugar levels in a healthy range, the next step is medication, usually insulin injections. This will help keep blood glucose levels low and poses little risk to the baby because insulin does not pass through the placenta.
Changes to pregnancy care
With a GDM diagnosis, a pregnancy is typically considered higher risk. It will likely require more frequent prenatal checkups and additional ultrasound scans to monitor the baby’s growth.
Health care practitioners may recommend early induction to avoid the baby growing too large. However, studies have shown that induction before 39 weeks does not improve outcomes for pregnancies affected by gestational diabetes, and may even increase the risk of a C-section birth.
What is the connection between GDM and later diabetes diagnoses?
According to Real Food for Gestational Diabetes, previously reviewed by Natural Womanhood, up to 70% of women who are diagnosed with GDM are also diagnosed with type 2 diabetes within five years of giving birth. The ADA recommends screening for diabetes 4 to 12 weeks postpartum, and up to a third of women test positive for prediabetes or type 2 diabetes at this time. Regular screening every 1 to 3 years is also recommended for anyone with a past GDM diagnosis. This doesn’t necessarily mean that having gestational diabetes causes chronic diabetes to develop. It’s more likely that a gestational diabetes diagnosis identifies preexisting insulin resistance or prediabetes.
The ADA recommends screening for diabetes 4 to 12 weeks postpartum, and up to a third of women test positive for prediabetes or type 2 diabetes at this time. Regular screening every 1 to 3 years is also recommended for anyone with a past GDM diagnosis.
In such cases, receiving a gestational diabetes diagnosis may actually be an early warning to women with an underlying health issue that allows them to take action to protect their health. Research has shown that when women who have had gestational diabetes make lifestyle changes, they are much less likely to develop high blood pressure or type 2 diabetes.
Can you prevent gestational diabetes?
It depends, but eating well and exercising are the best ways to minimize risk factors like prediabetes before getting pregnant. And since implementing healthy lifestyle changes is harder than ever during pregnancy amidst morning sickness, cravings, and fatigue, it’s best to form those habits sooner rather than later.
If you are already pregnant, you can lower your risk of developing GDM by following similar nutritional guidelines as you would for insulin resistance outside of pregnancy—namely, focusing on getting plenty of protein and healthy fats, and limiting high-glycemic carbs. On the other hand, foods that are highly processed or contain a lot of sugar will contribute to high blood sugar and insulin resistance, increasing your risk of gestational diabetes.
GDM-preventing nutrition isn’t just about limiting carbs, though. In her blog post “9 Myths About Gestational Diabetes,” Lily Nichols points to evidence that eating adequate protein early in pregnancy provides crucial amino acids to the pancreas, supporting its work pumping out insulin later in pregnancy.
Earlier testing may not prevent GDM but can allow for proactive treatment
Most women aren’t screened for gestational diabetes until late in the second trimester of pregnancy, which doesn’t leave them much time to address high blood sugar if they receive a diagnosis. There are, however, ways to test for high blood sugar in early pregnancy, before the typical onset of insulin resistance.
One way is to test A1c levels in the blood. An A1c level of 5.7% or higher predicts gestational diabetes up to 99.8% of the time. While this knowledge won’t reverse gestational diabetes, it can allow women to make lifestyle changes much earlier in pregnancy that lower the risk of complications. If your healthcare practitioner doesn’t automatically test A1c, it can easily be added to a blood panel.
Another way to get clued in on blood sugar levels is with a continuous glucose monitor (CGM). Since a CGM tracks blood sugar levels continuously, it has the advantage of allowing you to see how your blood sugar levels fluctuate throughout the day and in response to eating different foods. CGMs are becoming more widely available, even without a prescription, though you may find it helpful to work with an experienced healthcare professional or nutritionist to interpret the data it collects and give personalized advice.
Why conventional nutritional advice for GDM falls short
In recent years, researchers have begun to call into question the amount of carbohydrates that pregnant women are recommended to consume after a GDM diagnosis. While groups such as the ADA recommend that carbs make up no more than a quarter of any given meal, the Institute of Medicine’s official guidelines state that pregnant women should consume at least 175g of carbs daily. The reason for having a minimum carb intake level is to ensure that women are eating enough to support a developing baby.
However, in developed countries like the US, the average daily carb intake of a pregnant woman is estimated to be a whopping 270 grams. It has also been estimated that pregnant women in the US consume fifteen percent of their total daily calories as added sugars, from sources like soda that have no nutritional value. What these statistics suggest is that a greater focus is needed on limiting carb intake during pregnancy, rather than setting an unbounded minimum.
Instead, nutrition experts like Nichols have argued that getting enough protein with every meal, throughout pregnancy (with or without GDM!), should be the foundation of prenatal nutrition. Proteins are vital to the growth of the baby and also help regulate blood sugar. Adequate protein intake has been estimated at 80-100 grams per day, yet the recommended daily intake falls far short of this, at 46g/day during the first trimester and 71g/day during the second and third trimesters [5].
A promising development for nutritional guidelines during pregnancy came with the new Dietary Guidelines released by the federal government. The guidelines cited evidence supporting higher protein intake outside of pregnancy, in the range of 1.2-1.6 g/kg per day (which translates to 82-109g of protein per day for a woman who weighs 150 pounds). The guidelines also acknowledge that protein needs increase during pregnancy, though no exact amounts were specified.
The bottom line
GDM can pose serious risks for a pregnancy and the long-term health of a mother and her baby, but these are risks, not certainties. Whether you’ve already received a GDM diagnosis or aren’t even pregnant yet, the first and best step to keeping yourself and your baby healthy is to eat nourishing food and make regular moderate exercise part of your lifestyle.
