A 2024 research study conducted jointly by Northwestern University and University of Texas Southwestern Medical Center calls into question the ways reproductive hormone levels respond to oral contraception.
Mainstream medical sites have long claimed that hormonal contraceptives (of which birth control pills are the most common type) “regulate” the menstrual cycle by “introducing hormones into the body at a steady pace.”
Here at Natural Womanhood, we’ve explicado anteriormente why hormonal contraceptives do no regulate the cycle, and how a cycle on the pill is no cycle at all. We used the term “flatline” to describe what happens to your hormone levels on the pill.
But were all of us wrong?
What we thought hormonal contraceptives did to women’s hormone levels
Nosotros previously wrote that synthetic estrogen (EE) and progestin, as found in combined hormonal contraceptives, acted on your hypothalamic-pituitary-ovarian axis, or HPO axis (the brain-ovary communication pathway that directs your menstrual cycle), and tanked your body’s own estrogen (E) and progesterone levels to prevent ovulation.
We wrote, “This lowers the body’s natural estrogen and progesterone, to levels below which ovulation cannot occur… the Pill induces a ‘flatline’ for FSH, LH, estrogen and progesterone.”
We included an image from a 2018 research study which did not cite the specific studies used to generate the graph, but which reflected the general scientific consensus on how hormonal contraceptives affect endogenous hormonal production. Based on what we explained, one would espere that natural estrogen and progesterone levels would remain relatively stable for the first 21days of the cycle, before increasing during the placebo pill week.
(Athletic performance and the oral contraceptive – PubMed, Oral contraceptive phase has no effect on endurance test – PubMed, Examining the role of oral contraceptive users as an experimental and/or control group in athletic performance studies – PubMed)
We did not address patterns in synthetic estrogen or progestin levels.
What hormonal contraceptives actually do to women’s hormone levels
What we were right about
It’s true that a cycle on the pill is no a regular menstrual cycle, and the bleeding you get during placebo week is a withdrawal bleed and not your period. Remember, a true period follows ovulation.
We were also right that, below a certain threshold, estrogen and progesterone levels will not support ovulation, or implantation if ovulación intercurrente and conception occur.
What we didn’t know
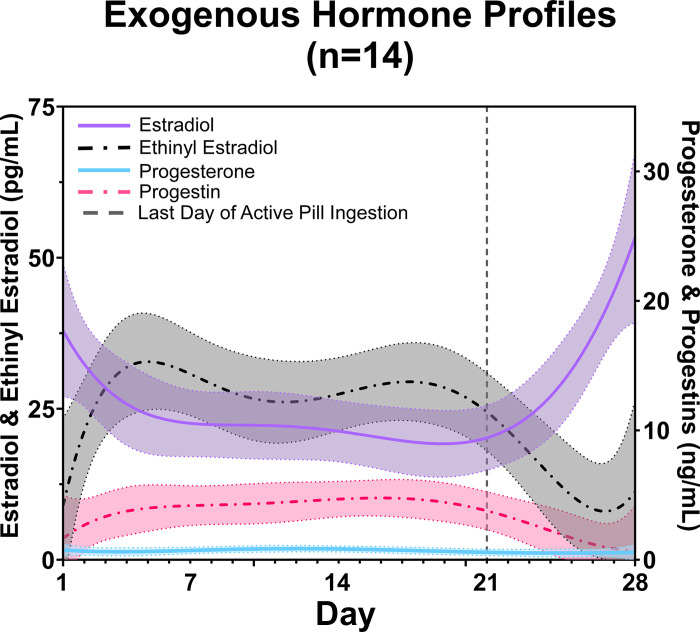
What we wrote was correct as far as it went. But the Estudio 2024 tracked the body’s own hormone levels y artificial hormone levels via blood draws from 14 healthy participants, every other day for a whole pill pack, or 28 days. Natural hormones estrogen and progesterone were tested with a competitive enzyme immunoassay. Synthetic hormones ethinyl estradiol and progestin were measured via liquid chromatography-mass spectrometry (more on this below).
Here’s what researchers found.
Estrogen levels fluctuate
To be clear, the body’s natural estrogen is estradiol or E (while the body makes four kinds of estrogen, estradiol is the most common and bioactive form in women of reproductive age) and the synthetic estrogen found in oral contraception is ethinylestradiol (EE).
Rather than remaining flat throughout the active pill days, E and EE levels both varied across the cycle (pictured aquí). By seven days after the start of the placebo pills, the average E level had risen by over 30 points from the average level during the middle of the active pill pack. This makes sense because without the E suppression caused by the artificial EE from the pills, the body’s own E production would be expected to naturally rise.
But there was still variability even across the active pill days. In fact, while the researchers did not comment on this, the highest levels of E on two cycle days (days 2 and 12, pictured in Table 2) would indicate potential fertility (and therefore the possibility of conception if the user had sex on that day) incluso while women were taking the active pills.
Interestingly, participants using a birth control pill brand with relatively lower EE dosage had a defined increase in E (natural estrogen) after the placebo pill week. But participants using a brand with relatively higher EE dosage had a smaller E rise after the placebo pills. Fascinatingly, these same women taking relatively higher daily doses of EE also had more variable EE levels over the course of the 28 days.
Progesterone levels did not fluctuate
In contrast, the body’s own progesterone levels did not meaningfully change at any point during the pill pack, whether during days of active pill intake or placebo pill intake. This behavior more closely represents the “flatline” we described previously. The progestin (artificial progesterone from the birth control pill) levels increased starting on day 1, and remained high until the placebo pill week started, at which point levels dropped significantly.
The grain of salt
Only 14 women participated in the 2024 research study, which is fairly typical of women’s health research and/or testing of new therapies or interventions. Much larger sample sizes are needed to corroborate the results.
What’s more, the participants were healthy women, whereas many oral contraceptive users are not. Further scientific exploration is needed to identify whether common conditions like metabolic syndrome, endometriosis or PCOS affect the way hormonal contraceptives influence natural hormone levels.
How did previous research miss the way women’s hormones behave on the pill?
The savvy reader or curious observer might ask how decades of women’s health research missed the way women’s own (endogenous) hormones fluctuate on the pill. For those ready to dive into the weeds, the researchers summarize the main reasons this may be the case. In brief, issues with the “gold standard” hormone testing method, use of ‘snapshot in time’ testing instead of testing multiple times over the course of a whole cycle, and measuring either the body’s own hormones or artificial hormone levels rather than both.
Why this matters for women’s health research
Historically, naturally cycling women were considered “too complicated” to study because of the fluctuations in their reproductive hormones over the course of a cycle or study period. The researchers wrote, “At present, women on hormonal contraceptives, particularly combination monophasic oral contraceptive (CMOC), are considered a ‘control’ group in many studies based on the assumption that their hormonal milieu is comparable and consistent (10, 22, 23)."
Women taking hormonal contraceptives have been preferred because, as the research study noted, “The rationale is that women chronically exposed to exogenous hormones in contraceptives will have stable and similar concentrations of both endogenous and exogenous hormones (9, 10)."
But the 2024 research study found that, even while on hormonal contraception, women’s endogenous and exogenous hormone levels fluctuate more than we thought. All the more reason for women’s health research to include naturally cycling women.
The 2024 research study found that, even while on hormonal contraception, women’s endogenous and exogenous hormone levels fluctuate more than we thought. All the more reason for women’s health research to include naturally cycling women.
Lo esencial
Of course, some will insist that the hormonal fluctuations on the pill simply mean that the monthly ‘pill pause’ should be eradicated, and users should take active hormonal contraception continuously—without placebo pills.
Here at Natural Womanhood, we will continue to advocate for healthier options for family planning and/or reproductive health treatments that don’t compromise women’s mental or physical health, or cause them to miss out on the known beneficios de la ovulación para la salud.